
سر فصل مطالب
تی ام اس rTMS درمان میگرن ، افسردگی و بیماری پارکینسون

Shweta Gupta, Shashi Kumar Singh, Birendra Chauhan
درمان تحریک مغناطیسی ترانس کرانیال یا همان تی ام اس rTMS درمان میگرن، افسردگی و بیماری پارکینسون را به جدیدترین روش درمان نورولوژیکی و روانپزشکی ، انجام میدهد .
اساسا این درمان شامل پالس های مغناطیسی است که به جای جریان الکتریکی مستقیم باعث فعال شدن مغز می شود. سیم پیچ یا کویل روی سر بیمار قرار می گیرد و پالس های الکترومغناطیسی کوتاه از سیم پیچ عبور می کند و روی سر فرد یک میدان مغناطیسی ایجاد می کند که منجر به تغییر می شود.
پالس مغناطیسی براحتی از جمجم عبور می کند و منجر به تحریکات الکتریکی کوچکی در سلولهای ناحیه ی هدف در مغز، می شود. این جریان تا حدود 2 اینچ در داخل مغز نفوذ می کند. این میدان مغناطیسی قدرتی مشابه تصویر برداری رزونانس مغناطیسی (MRI)دارد.
مقدمه
درمان تحریک مغزی شامل فعال کردن مستقیم مغز بوسیله ی الکتریسیته، مغناطیس یا ایمپلنت برای درمان افسردگی و سایر اختلالات است. سایر درمان های تحریکی شایع عبارتند از: تحریک عصب واگ، تحریک عمقی مغز، درمان مغناطیسی تشنج.
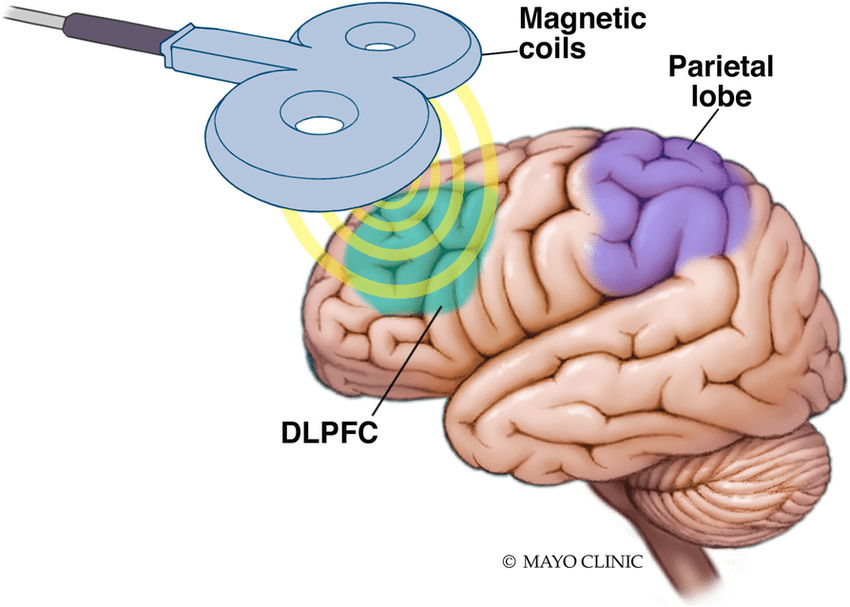
تحریک مغناطیسی مکرر فراجمجمه ای شامل هدف قرار دادن مناطقی از مغز است که در افسردگی یا سایر بیماری های خلقی درگیر می شوند در این روش می توان به صورت انتخابی مناطق کوچکی از مغز را دستکاری کرد یا تغییراتی در فعالیتشان ایجاد کرد. میدان مغناطیسی از کویل که به شکل 8 است عبور می کند.
این کویل، سیمی با روکش پلاستیکی دارد که اجازه می دهد میدان مغناطیسی بر منطقه ی خاصی از کرتکس یا سطح مغز،متمرکز شود. میدان مغناطیسی تولید شده توسط TMS می تواند از پوست سر و جمجمه عبور کند و بدون اینکه دردی تولید کند تحریکاتی در نورون های مغزی ایجاد کند.
از آنجایی که این تحریکات مغزی در فواصل منظمی تولید شود به آن تحریکات مکرر مغناطیسی یا rTMS می گویند. پارامترهای تحریک از جمله تعداد ، قدرت، مدت تحریک و نیز فاصله بین تحریکات می تواند متغیر باشد.
قابلیت تغییر در پارامترهای درمان در مناطق مختلف مغزی نشان می دهد که این درمان قابلیت زیاد و پتانسیل درمان خوبی دارد و می تواند برای هر فرد متناسب با بیماری طراحی شود.
کلینیک تخصصی مغز و اعصاب و روان ذهن برتر ایرانیان بعنوان بنیانگذار درمان rTMS (تی ام اس) در کشور و دارای پروانه رسمی وزارت بهداشت و درمان و آموزش پزشکی می باشد که این مرکز خدمات درمانی rTMS توسط به روزترین تجهیزات و با تعرفه مصوب می باشد. برای مشاهده تعرفه خدمات تی ام اس rTMS در اینجا کلیک کنید.
عملکرد rTMS
rTMS با استفاده از آهنربای مغناطیسی قرار گرفته بر روی پوست سر میدان مغناطیسی تقریبا برابر با قدرت MRI تولید می کند. پالس مغناطیسی بخش کوچکی از سطح مغز را تحریک می کند. فرکانس پایین (یک بار در هر ثانیه) منجر به کاهش در فعالیت آن بخش از مغز می گردد.
تحریک مغناطیسی فراجمجمه ای توسط یک تخلیه سریع جریان از یک خازن بزرگ در کویل که میدان مغناطیس 1 تا 10 میلی تسلا تولید می کند، ایجاد می شود. این جریان مغناطیسی می تواند منطقه ی هدف را دپولاریزه یا هایپرپولاریزه کند. بر اساس قانون معادله ماکسل – فارادی است:
این جریان باعث تغییر در غشا سلول می شود که منجر به دپولاریزه یا هایپرپولاریزه شدن سلول و و تولید پتانسیل عمل شود.
طول مدت rTMS
بستگی به پروتکل درمانی/ پژوهشی دارد؛ اما معمولا هر جلسه 20 قیقه است. تعداد جلسات هم با توجه به پروتکل متغیر است اما بسیاری به 10 الی 15 جلسه 5 بار در هفته نیاز دارند.
ویژگی های rTMS
- rTMS دارای ویژگی های منحصر به فرد زیادی است
- غیر تهاجمی است و براحتی می تواند روی منطقه ی کوچکی از مغز متمرکز شود، می تواند در نواحی انتخابی کرتکس مغز تغییر ایجاد کند این می تواند امکان بسیار خوبی برای درمان اختلالات مغزی مختلف باشد بعلاوه این روش اثرات جانبی را به حداقل می رساند.
- rTMS نشان داده است که می تواند برای شمار زیادی از اختلالات روانپزشکی که به درمان های داوریی و سایر درمان های شایع مقاوم هستند مفید باشد.
- rTMS می تواند برای برخی بیماران که نمی توانند دارو مصرف کنند مفید باشد.
- این روش می تواند برای بیماری های زیر مفید باشد:
-افسردگی
-افسردگی واسکولار (افسردگی ناشی از سکته)
-میگرن
-توهمات شنوایی مقاوم در اسکیزوفرنی
-افسردگی های مرتبط با بیماری پاکینسون
-اختلال استرس پس از سانحه
-اسکیزوفرنی با علائم منفی
– وزوز گوش مزمن
اثرات rTMS بر مغز
نحوه اثر rTMS در مغز هنوز کاملا مشخص نیست. اثرات این درمان می تواند بسته به نوع تحریک به دو گروه تقسیم شود: تک پالس یا paired پالس که می تواند نورون را در نئوکرتکس دپولاریزه کند و پتانسیل عمل ایجاد کند. اگر در کرتکس حرکتی اولیه استفاده شود.
فعالیت عضلانی تحت عنوان پتانسیل حرکتی برانگیخته (MEP) تولید کند که با الکترومیگرافی قابل ثبت است. اگر در ناحیه ی کرتکس پس سری استفاده شود منجر به ادراک فسفون (نور چشمک زن) می شود. در اغلب مناطق دیگر کرتکس تجربه هشیارانه ایجاد نمی شود.
اما تغییرات کمی در رفتار فرد ایجاد می کند ( به عنوان مثال زمان واکنش کندتر در تکالیف شناختی). تحریک مغناطیسی می تواند تاثیرات بلند مدت مقاوم ایجاد کند می تواند تحریک پذیری را با توجه به فرکانس و شدت تحریک و جهت کویل کاهش یا افزایش دهد. مکانیزم اثر هنوز مشخص نیست تعداد زیادی از افراد بر این باورند که نتایج بازتابی از تغییرات سیناپسی و تغییرات در long-term potentiation (LTP) و long-term depression (LTD) است.
متن اصلی مقاله
Repetitive Transcranial Magnetic Stimulation (RTMS) for the Treatment of Depression, Migraine and Parkinson’s Disease
1Shweta Gupta, 1Shashi Kumar Singh, 2Birendra Chauhan 1Electronics and Communication Department, Dr. K.N. Modi niversity affiliated to Rajasthan University, District Tonk,Rajasthan 2Mathematics Department, Dr. K. N. MIET, Modinagar*Corresponding author Shweta Gupta
Abstract: Repetitive transcranial magnetic stimulation (RTMS) is newest methodology for treatment of various
neurological and psychiatric disorders including migraine, stroke, Parkinson’s disease ,dystonia, tinnitus and depression.
It basically involves induction of electromagnetic pulses instead of electrical current to activate the brain.
An electromagnetic coil is held against the forehead and short electromagnetic pulses are administered through the coil using
a rapidly changing magnetic field. The magnetic pulse easily passes through the skull, and causes small electrical
currents that stimulate nerve cells in the targeted brain region.
This type of pulse generally does not reach further than two inches into the brain. The magnetic field is about the same strength as that of a magnetic resonance imaging (MRI)scan.
Keywords: Parkinson’s disease, depression, migraine, repetitive transcranial magnetic stimulation.
INTRODUCTION
Brain stimulation therapies involve activating
or touching the brain directly with electricity, magnets,
or implants to treat depression and other disorders.
Other stimulation therapies prevalent are — vagus
nerve stimulation, magnetic seizure therapy, and deep
brain stimulation.
Repetitive Transcranial Magnetic
Stimulation (rTMS) involves targeting specific areas of
brain that are believed to be affected by depression and
other mood disorders.
It has the ability to selectively
modulate or change activity in small areas of the brain
[1-2].
Treatment influences the electrical activity in
the brain by means of a pulsed magnetic field.
The magnetic field is generated by passing brief current
pulses through a figure-8 coil of wire [3].
This coil of wire is encased in plastic and held close to the scalp so
that the magnetic field can be focused onto specific
areas of the cortex, or surface, of the brain.
The magnetic field that is generated in rTMS can penetrate
the scalp and skull safely and painlessly to induce a
current in specific neurons (brain cells).
Because the magnetic stimulation is delivered at regular intervals, it
is termed repetitive TMS, or rTMS. Stimulation
parameters, such as the number of stimuli, the strength
of the stimuli, the duration of the stimuli, and the length
of the interval between stimuli can all be varied [4].
The ability to change parameters while directly targeting
specific brain cells suggests that rTMS therapy has an
extremely valuable therapeutic potential and treatment can be customized for each patient.
Fig-1: Eight shaped RTMS Device
WORKING OF RTMS
Transcranial magnetic stimulation (TMS) utilizes an electromagnet placed on the scalp that generates magnetic field pulses roughly the strength of an MRI scan. The magnetic pulses stimulate a small area on the surface of the brain about the size of a Shweta Gupta et al., Sch. J. Eng. Tech., 2014; 2(3C):488-490489
quarter. Low frequency (once per second) TMS has been shown to induce small, sustained reductions in activity in the part the rain that has been stimulated[5].
Fig. 2 RTMS Device in operation From the Biot-Savart Law… [1]
it has been shown that a current through a wire generates a magnetic field around that wire.
Transcranial magnetic stimulation is achieved by quickly discharging current from a large capacitor into a coil to produce pulsed magnetic fields of 1-10 mT [6,7]
By directing the magnetic field pulse at a targeted area of the brain, one can either depolarize or hyperpolarize neurons in the rain.
The magnetic flux density pulse generated by the current pulse through the coil causes an electric field due to the Maxwell-araday equation,… [2]
This electric field causes a change in the transmembrane current of the neuron, which leads to the depolarization or yperpolarization of the neuron and the firing of an action potential [8]
DURATION OF RTMS
It depends on the treatment/research protocol, but generally each session takes about 20 minutes. Treatment protocols vary in uration, but most require at approximately 10-15 sessions given five times per week [9].
PROPERTIES OF RTMS
1. RTMS has some very unique properties.
2. It is non-invasive, can easily be focused on small areas of the brain, and can modulate the brain cortex at selected site. This makes it particularly well suited for treating several brain disorders, while minimizing side effects [10].
3. rTMS has been shown to be effective in several psychiatric disorders not responding with currently available medication and ther therapies [11].
4. The rTMS can be also useful in some patients who are not able to take medications [12].
5. The techniques can be used in the following conditions:
1. Depression
2.Vascular Depression (Depression because of stroke).
3. Obsessive compulsive disorder
4. Migraine
5.Resistant auditory hallucination in Schizophrenia
6. Depression associated with parkinsonism disease
7. Post traumatic stress disorder
Schizophrenia with negative symptoms Chronic tinnitus
EFFECTS ON THE BRAIN The exact details of how TMS functions are still being explored. The effects of TMS can be divided into two types depending on the mode of stimulation:
Single or paired pulse TMS causes neurons in the neocortex under the site of stimulation to depolarize and discharge an action otential. If used in the primary motor cortex, it produces muscle activity referred to as a motor evoked potential (MEP) which an be recorded on electromyography [13-14].
If used on the occipitalcortex, ‘phosphenes’ (flashes of light) might be perceived by the subject. In most other areas of the cortex, the participant does not consciously experience any effect, but his or her behaviour may be slightly altered (e.g., slower reaction time on a cognitive task)
or changes in brain activity may be detected using sensing equipment [15-16].
Repetitive TMS produces longer-lasting effects which persist past the initial period of stimulation. rTMS can increase or decrease the excitability of the corticospinal tract depending on the intensity of stimulation, coil orientation, and frequency[17,18].
The mechanism of these effects is not clear, though it is widely believed to reflect changes in synaptic efficacy akin to long-term otentiation (LTP) and long-term depression (LTD) [19-20].
CONCLUSION
Thus, we have successfully studied RTMS and its various effects and diseases it can combat.
Shweta Gupta et al., Sch. J. Eng. Tech., 2014; 2(3C):488-490490
REFERENCES
1. Hoffman RE., Boutros NN, Hu S, Berman RM,
Krystal JH, Charney DS; Transcranial magnetic
stimulation and auditory hallucinations in
schizophrenia.” Lancet, 2000; 355(9209): 1073-
1075.
2. Hoffman RE, Hawkins KA, Gueorguieva R,
Boutros NN, Rachid F, Carroll K., Krystal JH;
Transcranial magnetic stimulation of left
temporoparietal cortex and medication-resistant
auditory hallucinations. Archives of General
Psychiatry, 2003; 60(1): 49-56.
3. Hoffman RE, Gueorguieva R, Hawkins KA,
Varanko M, Boutros NN, Wu YT, Carroll K,
Krystal JH; Temporoparietal transcranial magnetic
stimulation for auditory hallucinations: safety,
efficacy and predictors in a fifty patient sample.
Biological Psychiatry, 2005; 58(2):97-104.
4. Hoffman RE, Hampson M, Wu K, Anderson A,
Gore J, Buchanan RJ, Constable T, Hawkins K,
Sahay N, Krystal JH; Probing the pathophysiology
of auditory hallucinations by combining functional
magnetic resonance imaging and transcranial
magnetic stimulation. Cerebral Cortex,
2007;17(11):2733-2743.
5. Hoffman RE, Anderson A, Varanko M, Gore J,
Hampson M; The time course of regional brain
activation associated with onset of auditory/verbal
hallucinations. British Journal of Psychiatry, 2008;
193(5): 424-425.
6. World Health Organization. Depression fact sheet
No.369.
http://www.who.int/mediacentre/factsheets/fs369/e
n/index.html. Accessed February 27, 2013.
7. World Health Organization. The global burden of
disease: 2004 Available online at
http://www.who.int/healthinfo/global_burden_dise
ase/2004_report_update/en/index.html. Accessed
March 12, 2013.
8. Stahl SM; Stahl’s Essential Psychopharmacology:
Neuroscientific Basis and Practical Applications.
3rd ed. New York, NY: Cambridge University
Press (2008).
9. Janicak PG, O’Reardon JP, Sampson SM, Husain
MM, Lisanby SH, Rado JT, Heart KL, Demitrack
MA; Transcranial magnetic stimulation in the
treatment of major depressive disorder: a
comprehensive summary of safety experience from
acute exposure, extended exposure, and during
reintroduction treatment. J Clin Psychiatry, 2008;
69(2):222-232.
10. O’Reardon JP, Solvason HB, Janicak PG, Sampson
S, Isenberg KE, Nahas Z, et al; Efficacy and safety
of transcranial magnetic stimulation in the acute
treatment of major depression: a multisite
randomized controlled trial. Biol Psychiatry, 2007;
62(11):1208-1216.
11. George MS, Lisanby SH, Avery D, McDonald
WM, Durkalski V, Pavlicova M, et al; Daily left
prefrontal transcranial magnetic stimulation
therapy for major depressive disorder: a shamcontrolled
randomized trial. Arch Gen Psychiatry,
2010; 67(5):507-516.
12. Carpenter LL, Janicak PG, Aaronson ST, Boyadjis
T, Brock DG, Cook IA, et al; Transcranial
magnetic stimulation (TMS) for major depression:
a multisite naturalistc, observational study of acute
treatment outcomes in clinical practice. Depress
Anxiety, 2012; 29(7):587-596.
13. Avery DH, Isenberg KE, Sampson SM, Janicak
PG, Lisanby SH, Maixner DF, et al; Transcranial
Magnetic Stimulation in the acute treatment of
major depressive disorder: clinical response in an
open-label extension trial. J Clin Psychiatry, 2008;
69(3):441-451.
14. McDonald WM, Durkalski V, Ball ER,
Holtzheimer PE, Pavlicova M, Lisanby SH, et al;
Improving the antidepressant efficacy of
transcranial magnetic stimulation: maximizing the
number of stimulations and treatment location in
treatment-resistant depression. Depress Anxiety,
2011; 28(11):973-980.
15. Janicak PG, Nahas Z, Lisanby SH, Solvason HB,
Sampson SM, McDonald WM, et al; Durability of
clinical benefit with transcranial magnetic
stimulation (TMS) in the treatment of
pharmacoresistant major depression: assessment of
relapse during a 6-month, multisite, open-label
study.” Brain Stimulation, 2010; 3(4):187-199.
16. Demitrack MA, Thase ME; Clinical significance of
transcranial magnetic stimulation (TMS) in the
treatment of pharmaco resistant depression:
synthesis of recent data. Psychopharmacol Bull,
2009; 42(2):05-38.
17. Kito S, Fujita K, Koga Y; Changes in regional
cerebral blood flow after repetitive transcranial
magnetic stimulation of the left dorsolateral
prefrontal cortex in treatment-resistant depression.
J Neuropsychiatry Clin Neurosci, 2008; 20(1):74-
80.
18. World Health Organization. The World Health
Report 2001: Mental Health: New Understanding,
New Hope. Available online at
www.who.int/whr/2001/en/whr01_en.pdf.
19. Kessler RC, Berglund P, Demler O, Jin R, Koretz
D, Merikangas KR, et al; Epidemiology of major
depressive disorder: results from the National
Comorbidity “Survey Replication (NCS-R).
JAMA, 2003; 289(23):3095-3105.
20. World Health Organization. The ICD-10
classifications of mental and behavioural disorders:
clinical descriptions and diagnostic guidelines.
Available online at